November bimonthly assessment
1) 55 year old male patient came with the complaints of Chest pain since 3 days , Abdominal distension since 3 days and decreased urine output since 3days and not passed stools since 3days
https://sreejaboga.blogspot.com/2020/11/is-online-e-log-book-to-discuss-our.html?m=1
a) Where are the different anatomical locations of the patient's problems and what are the different etiologic possibilities for them? Please chart out the sequence of events timeline between the manifestations of each of these problems and current outcomes.
A) acute kidney injury secondary to pancreatitis
B) tibial - diaphysial dysplasia
C) Atherosclerotic vascular changes in right upper limb due to triglyceridemia
D) pancreas - acute severe pancreatitis secondary to call stones
E) lungs - pleural effusion secondary to acute severe pancreatitis
Sequence of events
1 ) Patient has atherosclerotic vascular disease in right upper limb
2) PT has c/o constipation , shortness of breath , chest pain , abd distension
3) As PT tlc were high he was started on antibiotics , after one more day he was in altered sensorium , then he was taken up dialysis and later his sensorium improved
4) later PT was taken up another session of dialysis but his tlc were high
a1) Added 17/11/2020 Mention the optimal diagnostic interventions in the patient done and that you may further order in a low resource setting to fathom the etiologic possibilities.
To look for pancreatitis and other complications of it , a CECT abdomen would very helpful
B) what are pharmacological and non pharmacological interventions used in the management of this pt and what are efficacy of each one of them ?
Iv fluids are given to maintain intravascular volume
And IV antibiotics usually given , if there is any infecred necrosis .
Non pharmacological interventions :
Ryles tube feeding , with standard precautions . It can given bedside to patient
2) A 55 year old male, shepherd by occupation, presented to the OPD with the chief complaints of fever (on and off), loss of appetite, headache, body pains, generalized weakness since 2 months, cough since 2 weeks and vomitings and pain abdomen since 2 days.
https://aakansharaj.blogspot.com/2020/11/55-year-old-male-with-anemia.html?m=1
a) Where are the different anatomical locations of the patient's problems and what are the different etiologic possibilities for them? Please chart out the sequence of events timeline between the manifestations of each of these problems and current outcomes
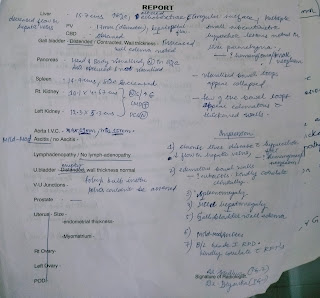
Pt has Anemia , acute renal failure , lytic bony leisons , cxr and sputum reports showing pneumonia
Anemia with low retic count ,Total proteins (12.4 g/dl) ,albumin (1.84 g/dl) high gamma gap ,
Differential diagnosis : Multiple myeloma
Multiple myeloma is a plasma cell dyscrasia ,where there are clone of plasma cells causing excessive production of immunoglobulins ,but these immunoglobulins are defective hence confer no immunity and these people are prone for more infections .
Multiple myeloma (MM) is a clonal plasma cell proliferative disorder characterized by the abnormal increase of monoclonal paraprotein leading to evidence of specific end-organ damage.
1. Due to bone marrow infiltration there is anemia , leucopenia
2. Lytic bony lesions on skull ( pepper pot skull )
3. Renal failure - Excess monoclonal immunoglobulin can cause hyperviscosity, platelet dysfunction and renal tubular damage, leading respectively to neurologic derangement, bleeding, and renal failure.
4. Head ache ,paresthesia and blurring of vision- are features of hyper viscosity.
5.lungs : Moderate to gross right pleural effusion and Multilobar consolidations of the right lung, involving upper and middle lobes With Passive collapse of basal segments of right lower lobe .
Sequence of events
-Alcohol & smoking (35 years)
-Stopped alcohol (4 years)
-Fever , generalised weakness & anemia - 2 units blood transfusion (1.5 years)
-Stopped smoking (4 months)
-Low grade fever , generalized weakness , headache , neck pain , loss of appetite , weight loss (2 months)
-Cough & SOB (2 weeks)
-Vomiting & pain abdomen (2 days)
B ) what are pharmacological and non pharmacological interventions used in the management of this pt and what are efficacy of each one of them ?
The preferred treatment for those under the age of 65 is chemotherapy, commonly with ,bortezomib based regimes and lenalidomide dexamethasone , followed by highdose therapy with melphalan , autologous hematopoietic stem cell graft .
3. 51 Year old man with complaints of B/L pitting pedal edema from 5 to 6months,abdominal distension from 2 to 3 days,SOB from 3days.
A) Where are the different anatomical locations of the patient's problems and what are the different etiologic possibilities for them? Please chart out the sequence of events timeline between the manifestations of each of these problems and current outcomes.
a. The macro and micro vascular complications are due to diabetes and hypertension
b. heart failure , diabetes , HTN are risk factors for AF
c . In AF there is stasis of blood which leads to clot formation and later gets dislodged which causes stroke
d. Left ventricular failure is due to HTN which causes pulmonary HTN which in turn causes right heart failure
SEQUENCE OF EVENTS:
- Tobacco chewing (40 years)
- Alcohol (10 years)
- DM (7 years)
- HTN (5 years)
- 1st Episode GTCS (3 years) & AF with HFpEF
- 2nd Episode GTCS (2 years)
- HFrEF & Anasarca (1 year) - (subsided with medication)
- Pedal edema (6 months)
- Increased pedal edema , abdominal distention , SOB and decreased urine output (3 days)
- Admitted
B ) what are pharmacological and non pharmacological interventions used in the management of this pt and what are efficacy of each one of them ?
Non pharmacological
Salt and fluid restriction will help improve symptoms of the PT
Pharmacological
Preload reducing agents - Diuretics (only if symptomatic)
Afterload reducing agents - vaso dilators ,ace inhibitors and arb
Beta blockers for preventing cardiac remodeling and reduce mortality.
Insulin for sugar control
4.) ) 31 yr old man with B/L pedal edema with scrotal and penile swelling since 2 months
https://nairaditya97.blogspot.com/2020/11/31-yr-old-male-with-bl-pedal-edema-with.html?m=1
A) Where are the different anatomical locations of the patient's problems and what are the different etiologic possibilities for them? Please chart out the sequence of events timeline between the manifestations of each of these problems and current outcomes.
1. .Patient is a chronic alcoholic which causes wet beri beri(heart failure due to thiamine deficiency)
2.peripheral neuropathy due to thiamine deficiency
EVENTS TIME LINE:
- Alcohol & khaini (3 years)
- Pins and needles (1 year)
- Palpitations and sob on exertion (8 months)
- PND (6months)
- Sexual disturbance and constipation (3months)
- Pedal edema and Scrotal edema(2 months)
- Admitted
B ) what are pharmacological and non pharmacological interventions used in the management of this pt and what are efficacy of each one of them ?
Thiamine for thiamine deficiency
Diuretics
Salt and fluid restriction
Comments
Post a Comment